RE© my wording and I am the original source for finding and detailing these HPV specific items transferred from my various files, e-mails, and postings.
Original E-mail I sent:
Mon 7/25/2016 12:52 PM
To:xxxx
This doesn't sound good, yeah what's in those virus like particles that would do this?:
Eur J Immunol. 2005 May;35(5):1548-56. http://www.ncbi.nlm.nih.gov/pubmed/15832296
Papillomavirus virus-like particles induce cytokines characteristic of innate immune responses in plasmacytoid dendritic cells.
Lenz P1, Lowy DR, Schiller JT.
Author information
Abstract
Human papillomavirus (HPV) virus-like particles (VLP) are being extensively tested as vaccines for the prevention of HPV-associated cervical cancer. Dendritic cells (DC) acquire and present antigens, initiating innate and adaptive immune responses. It has been shown previously that DC of the myeloid lineage are capable of generating adaptive immune responses to HPV VLP in vitro. However, the capacity of plasmacytoid DC (pDC) to acquire HPV VLP and the nature of the immune response generated have not been reported. In this study we found that freshly isolated as well as CpG-matured pDC bind papillomavirus VLP and that internalization occurs preferentially in the immature pDC. In contrast to myeloid DC, pDC did not undergo phenotypic maturation upon exposure to HPV16 VLP. However, HPV16 VLP induced pDC to secrete of IFN-alpha and IL-6, both cytokines that play a role in the generation of antibody responses, as well as TNFalpha and IL-8. Given that VLP do not contain viral nucleic acids, these results indicate that viral capsids alone may be capable of inducing cytokine production by pDC. Finally, CpG-activated pDC, but not pDC exposed to HPV16 VLP, activated lymphocytes to secrete IL-10 and low levels of IFN-gamma. Together these findings suggest a possible immunogenic effect of pDC in the setting of VLPvaccination.
They were working on the VLP's in 1993 for HPV:
Virol. 1993 Dec;67(12):6929-36.
Efficient self-assembly of human papillomavirus type 16 L1 and L1-L2 into virus-like particles.
Kirnbauer R1, Taub J, Greenstone H, Roden R, Dürst M, Gissmann L, Lowy DR, Schiller JT.
Author information
Abstract
The L1 genes of two human papillomavirus type 16 (HPV16) isolates derived from condylomata acuminata were used to express the L1 major capsid protein in insect cells via recombinant baculoviruses. Both L1 major capsid proteins self-assembled into virus-like particles (VLP) with high efficiency and could be purified in preparative amounts on density gradients. The yield of VLP was 3 orders of magnitude higher than what has been obtained previously, using L1 derived from the prototype HPV16. DNA sequence comparison identified a single nonconserved amino acid change to be responsible for the inefficient self-assembly of the prototype L1. VLP were also obtained by expressing L1 of HPV6, HPV11, and cottontail rabbit papillomavirus, indicating that L1 from a variety of papillomaviruses has the intrinsic capacity to self-assemble into VLP. Coexpression of HPV16 L1 plus L2 by using a baculovirus double-expression vector also resulted in efficient self-assembly of VLP, and the average particle yield increased about fourfold in comparison to when L1 only was expressed. Coimmunoprecipitation of L1 and L2 and cosedimentation of the two proteins in a sucrose gradient demonstrated that L2 was incorporated into the particles. The ability to generate preparative amounts of HPV16 L1 and L1-L2 VLP may have implications for the development of a serological assay to detect anti-HPV16 virion immune responses to conformational epitopes and for immunoprophylaxis against HPV16 infection.http://www.ncbi.nlm.nih.gov/pubmed/8230414
------------------------------------------
To:xxxx
This doesn't sound good, yeah what's in those virus like particles that would do this?:
Eur J Immunol. 2005 May;35(5):1548-56. http://www.ncbi.nlm.nih.gov/pubmed/15832296
Papillomavirus virus-like particles induce cytokines characteristic of innate immune responses in plasmacytoid dendritic cells.
Lenz P1, Lowy DR, Schiller JT.
Author information
Abstract
Human papillomavirus (HPV) virus-like particles (VLP) are being extensively tested as vaccines for the prevention of HPV-associated cervical cancer. Dendritic cells (DC) acquire and present antigens, initiating innate and adaptive immune responses. It has been shown previously that DC of the myeloid lineage are capable of generating adaptive immune responses to HPV VLP in vitro. However, the capacity of plasmacytoid DC (pDC) to acquire HPV VLP and the nature of the immune response generated have not been reported. In this study we found that freshly isolated as well as CpG-matured pDC bind papillomavirus VLP and that internalization occurs preferentially in the immature pDC. In contrast to myeloid DC, pDC did not undergo phenotypic maturation upon exposure to HPV16 VLP. However, HPV16 VLP induced pDC to secrete of IFN-alpha and IL-6, both cytokines that play a role in the generation of antibody responses, as well as TNFalpha and IL-8. Given that VLP do not contain viral nucleic acids, these results indicate that viral capsids alone may be capable of inducing cytokine production by pDC. Finally, CpG-activated pDC, but not pDC exposed to HPV16 VLP, activated lymphocytes to secrete IL-10 and low levels of IFN-gamma. Together these findings suggest a possible immunogenic effect of pDC in the setting of VLPvaccination.
They were working on the VLP's in 1993 for HPV:
Virol. 1993 Dec;67(12):6929-36.
Efficient self-assembly of human papillomavirus type 16 L1 and L1-L2 into virus-like particles.
Kirnbauer R1, Taub J, Greenstone H, Roden R, Dürst M, Gissmann L, Lowy DR, Schiller JT.
Author information
Abstract
The L1 genes of two human papillomavirus type 16 (HPV16) isolates derived from condylomata acuminata were used to express the L1 major capsid protein in insect cells via recombinant baculoviruses. Both L1 major capsid proteins self-assembled into virus-like particles (VLP) with high efficiency and could be purified in preparative amounts on density gradients. The yield of VLP was 3 orders of magnitude higher than what has been obtained previously, using L1 derived from the prototype HPV16. DNA sequence comparison identified a single nonconserved amino acid change to be responsible for the inefficient self-assembly of the prototype L1. VLP were also obtained by expressing L1 of HPV6, HPV11, and cottontail rabbit papillomavirus, indicating that L1 from a variety of papillomaviruses has the intrinsic capacity to self-assemble into VLP. Coexpression of HPV16 L1 plus L2 by using a baculovirus double-expression vector also resulted in efficient self-assembly of VLP, and the average particle yield increased about fourfold in comparison to when L1 only was expressed. Coimmunoprecipitation of L1 and L2 and cosedimentation of the two proteins in a sucrose gradient demonstrated that L2 was incorporated into the particles. The ability to generate preparative amounts of HPV16 L1 and L1-L2 VLP may have implications for the development of a serological assay to detect anti-HPV16 virion immune responses to conformational epitopes and for immunoprophylaxis against HPV16 infection.http://www.ncbi.nlm.nih.gov/pubmed/8230414
------------------------------------------
Original E-mail I sent:
Sent: Wednesday, July 27, 2016 9:40 AM
To: xxxxx
Subject: Fw: HPV Time line of events, patents, hpv is most expensive vax
Lowy's patent attached
------------------------------------------
Original E-mail I sent:
Sent: Wednesday, July 27, 2016 9:24 AM
Subject: HPV Time line of events, patents, hpv is most expensive vax
Time line of event's
HPV vax is the most expensive one and why they are attempting to mandate it throughout the US is that insurance will pay the high cost. They did all the research in developing countries where 85% of cervical cancer happens.
Here's a timeline on the HPV: This link is t Lowy's patent and the timeline link following
Table 1: Timeline of patenting and licensing of HPV L1-VLP–based prophylactic vaccines http://www.nature.com/nbt/journal/v28/n7/fig_tab/nbt0710-671_T1.html
Technologies underlying the L1-VLP based prophylactic vaccines emerged from research conducted at the University of Rochester, the NCI, Georgetown University and the University of Queensland. The NCI initially nonexclusively licensed the technology to MedImmune and Merck. MedImmune also acquired worldwide exclusive rights to IP from Georgetown University and the University of Rochester. The University of Queensland licensed its patents to CSL, which in turn licensed the technology exclusively to Merck. GSK eventually acquired exclusive rights to MedImmune's entire IP portfolio for HPV vaccine development. Owing to a first-to-invent system in the United States, patent interference proceedings were triggered at the USPTO when claims overlapped from different patent applications filed by four different groups of inventors. The interference proceedings involved various L1-antigen HPV-related claims. Six two-way patent interferences between the four parties continued for nearly a decade, presumably at significant cost to the institutions or their primary licensees, and were partially resolved in 2005. Given the uncertainty surrounding the ownership of enabling vaccine technologies and the possibility of mutually blocking exclusive rights (that is, neither firm could be sure its products would not infringe on patent rights held by the other), Merck and GSK cross-licensed their respective IP holdings in 2005 to ensure unfettered access to these technologies. They consequently secured their market position in the United States and Europe and other OECD nations such as Canada and Japan. As part of the financial settlement of the patent interference, the nonexclusive licenses awarded by NCI, NIH to MedImmune and Merck were converted to co-exclusive licenses, thus allowing both GSK and Merck access to this IP. Merck brought Gardasil to market in the United States in 2006 and Cervarix was introduced in the United Kingdom in June 2008.
USPTO, US Patent and Trademark Office; CAFC, US Court of Appeals for the Federal Circuit.July 19, 1991 Frazer et al. (Queensland) file international patent application in Australia
June 25, 1992 Schlegel et al. (Georgetown) file patent application in US
September 3, 1992 Schiller and Lowy et al. (NCI, NIH) file patent application in US
March 9, 1993 Rose et al. (Rochester) file patent application in US
February 1995 University of Queensland's commercial arm UniQuest licenses HPV vaccine technology to CSL (Melbourne)
October 5, 1995 MedImmune acquires exclusive license to HPV vaccine technology from University of Rochester
1995 Merck licenses HPV vaccine technology from CSL
June 26, 1996 MedImmune in-licenses key HPV IP from German Cancer Research Center
January 7, 1997 NCI non-exclusively licenses HPV vaccine technology to MedImmune
June 24, 1997 USPTO declares initial interference
December 1997 NCI nonexclusively licenses HPV vaccine technology to Merck
December 11, 1997 MedImmune and SmithKline Beecham form worldwide HPV vaccine alliance
January 16, 1998 MedImmune finalizes vaccine agreement with SmithKline Beecham
October 24, 2001 USPTO declares patent interference 104,771 between Rose and Lowy
USPTO declares patent interference 104,772 between Rose and Schlegel
USPTO declares patent interference 104,773 between Rose and Frazer
USPTO declares patent interference 104,774 between Lowy and Schlegel
USPTO declares patent interference 104,775 between Lowy and Frazer
USPTO declares patent interference 104,776 between Schlegel and Frazer
February 2005 Merck and GSK enter cross-license agreement for HPV patents
May 2005 NCI's nonexclusive licenses convert to co-exclusive licenses
September 20, 2005 USPTO Board of Interference announces decision and awards priority to Schlegelet al.
December 29, 2005 Frazer et al. appeal USPTO decision, case docketed in CAFC
August 20, 2007 CAFC reverses USPTO decision and awards priority to Frazer et al.
Intellectual property, technology transfer and manufacture of low-cost HPV vaccines in India
http://www.nature.com/nbt/journal/v28/n7/full/nbt0710-671.html
---------------------------------------------------
June 25, 1992 Schlegel et al. (Georgetown) file patent application in US
September 3, 1992 Schiller and Lowy et al. (NCI, NIH) file patent application in US
March 9, 1993 Rose et al. (Rochester) file patent application in US
February 1995 University of Queensland's commercial arm UniQuest licenses HPV vaccine technology to CSL (Melbourne)
October 5, 1995 MedImmune acquires exclusive license to HPV vaccine technology from University of Rochester
1995 Merck licenses HPV vaccine technology from CSL
June 26, 1996 MedImmune in-licenses key HPV IP from German Cancer Research Center
January 7, 1997 NCI non-exclusively licenses HPV vaccine technology to MedImmune
June 24, 1997 USPTO declares initial interference
December 1997 NCI nonexclusively licenses HPV vaccine technology to Merck
December 11, 1997 MedImmune and SmithKline Beecham form worldwide HPV vaccine alliance
January 16, 1998 MedImmune finalizes vaccine agreement with SmithKline Beecham
October 24, 2001 USPTO declares patent interference 104,771 between Rose and Lowy
USPTO declares patent interference 104,772 between Rose and Schlegel
USPTO declares patent interference 104,773 between Rose and Frazer
USPTO declares patent interference 104,774 between Lowy and Schlegel
USPTO declares patent interference 104,775 between Lowy and Frazer
USPTO declares patent interference 104,776 between Schlegel and Frazer
February 2005 Merck and GSK enter cross-license agreement for HPV patents
May 2005 NCI's nonexclusive licenses convert to co-exclusive licenses
September 20, 2005 USPTO Board of Interference announces decision and awards priority to Schlegelet al.
December 29, 2005 Frazer et al. appeal USPTO decision, case docketed in CAFC
August 20, 2007 CAFC reverses USPTO decision and awards priority to Frazer et al.
Intellectual property, technology transfer and manufacture of low-cost HPV vaccines in India
http://www.nature.com/nbt/journal/v28/n7/full/nbt0710-671.html
---------------------------------------------------
Original E-mail I sent:
Sent: Sunday, June 5, 2016 12:07 PM
Subject: HPV vax history - NIAID2007 vax Jordon report
Check out this 2007 Jordan Report from NIAID. Page 87 talks about NCI licensed the technology to Merck and Glaxo. So they base the 2 strains HPV 16and 18 on high risk groups and countries with little access to health care. These 2 researchers from NCI developed technology underlying the FDA-approved HPV vaccines. Dr. Douglas Lowy and Dr. John Schiller describe their quest for an HPV vaccine to aid in preventing cervical cancer at the National Institutes of Health (NIH) Intramural Researcher Program (IRP). More info on Dr. Lowy:
Dr. Lowy is being recognized for his key discoveries that led to development of the human papillomavirus (HPV) vaccine to prevent cancer. The vaccine developed by Dr. Lowy (in collaboration with Merck and GlaxoSmithKline), and approved by the FDA in 2006, was the first licensed vaccine to prevent cancer by guarding against the sexually transmitted infection that causes the disease.
So Dr. Lowy was involved with both these vaccines.
(Three vaccines are approved by the FDA to prevent HPV infection Merck did Gardasil and Glaxo-Smith Kline made Cervarix: Gardasil, Gardasil 9, and Cervarix. All three vaccines prevent infections with HPV types 16 and 18, two high-risk HPVs that cause about 70 percent of cervical cancers and an even higher percentage of some of the other HPV-associated cancers (9, 10). Gardasil also prevents infection with HPV types 6 and 11, which cause 90 percent of genital warts (17). Because Gardasil protects against infection with four HPV types, it is called a quadrivalent vaccine. Gardasil 9 prevents infection with the same four HPV types plus five additional high-risk HPV types (31, 33, 45, 52, and 58) and is therefore called a nonavalent, or 9-valent, vaccine. All three vaccines are given through a series of three injections into muscle tissue over a 6-month period.)
Human papillomavirus (HPV) is the name given to a group of viruses that includes more than 100 different strains. Almost every cervical cancer in the United States and abroad is caused by sexually transmitted infection with HPV. Two dominant strains of HPV, types 16 and 18, together cause 70 percent of new cases of cervical cancer. In 2006, a vaccine to prevent infection by these two HPV types was approved by the U.S. Food and Drug Administration (FDA). This vaccine, based primarily on technology developed by scientists from the National Cancer Institute’s (NCI) Center for Cancer Research, offers great hope for reducing the global burden of cervical cancer.
Dr. Lowy, who is involved in studies of both vaccines - See more at: http://www.curetoday.com/publications/cure/2006/special-issue2006/first-approved-hpv-vaccine-could-slash-number-of-cervical-cancers#sthash.0xFYfKLh.dpuf
Using molecular biology techniques, NCI scientists engineered a vaccine to prevent HPV infection. They demonstrated that the major HPV capsid protein by itself can self-assemble into non-infectious virus-like particles (VLPs) that are highly immunogenic. Immunization with these VLPs, which lack any infectious or oncogenic genetic material, stimulates production of large quantities of antibodies that prevent HPV virus infections in humans.
NCI licensed the technology to two pharmaceutical companies, Merck and GlaxoSmithKline (GSK), to develop HPV vaccines commercially. Both companies are running large-scale Phase III trials of their versions of an HPV vaccine. GSK’s targets the two most oncogenic HPV strains, 16 and 18. Merck’s vaccine also targets strains 16 and 18, as well as strains 6 and 11, which cause about 90 percent of genital warts. Phase II trials by both companies produced encourag Low-Risk and High-Risk HPVs. This chart shows the three groups of genital HPV strains. While the majority of infections with high-risk HPVs clear up on their own, a few can trigger cervical cancer over time. Courtesy of NCI ing results. The VLP vaccines were more than 90 percent effective at preventing infection with the virus that can lead to the development of premalignant cervical abnormalities. Studies to date have demonstrated that the vaccine prevents infection for up to four years after vaccination. Studies are under way to determine if a booster, in addition to the three initial intramuscular injections, will be necessary for long-term protection. Merck submitted an application for FDA approval and on June 8, 2006, Gardasil was approved as the first vaccine developed to prevent cervical cancer, precancerous genital lesions, and genital warts due to HPV types 6, 11, 16, and 18.
NCI’s involvement in optimizing HPV vaccine development continues. NCI scientists have developed the first high-throughput assay to enable HPV vaccine developers to monitor protective antibody responses long term, and test whether their new vaccines can induce potentially protective antibody responses against other strains of HPV.
In anticipation of FDA approval of HPV vaccines, the Gates Foundation announced in June 2005 that it would grant $12.9 million to the World Health Organization, the International Agency for Research on Cancer, Harvard University, and the Program for Appropriate Technology in Health to establish systems to ensure quality control in vaccine distribution, monitor the impact of different HPV vaccination strategies, and facilitate introduction of the vaccines worldwide.
Jordon Report - Accelerated Vaccines
https://www.niaid.nih.gov/sites/default/files/jordan2007.pdf
----------------------------------------------
Original E-mail I sent:
On May 22, 2016, at 1:46 PM
See the info below this first part for the pediatrics HPV stuff. Unger worked with Reeves and Vernon in CFS long ago
Posted: December 17, 2010
Elizabeth (Beth) Unger, PhD, MD, has been selected to serve as the Chief of the Chronic Viral Diseases Branch (CVDB) in the Division of High-Consequence Pathogens and Pathology (DHCPP), National Center for Emerging and Zoonotic Infectious Diseases (NCEZID), Centers for Disease Control and Prevention (CDC).
Dr. Unger has served as the Acting Chief of CVDB since January 2010 and has 13 years of experience in CVDB, where she has participated in the design and implementation of CFS research and HPV laboratory diagnostics.
During this time, she was co-author on 25 peer-reviewed manuscripts related to CFS, including the often-cited descriptions of the Wichita and Georgia population-based studies. In addition, Dr. Unger has been instrumental in efforts by WHO to establish an HPV LabNet and serves as lead of a WHO HPV Global Reference Laboratory.
She is co-author of 142 peer-reviewed publications and 24 book chapters and serves on the editorial board of six scientific journals. In 2008, for her HPV research accomplishments, she received the Health and Human Services (HHS) Career Achievement Award.
Dr. Unger received an undergraduate degree in Chemistry at Lebanon Valley College, Annville, PA. She then earned her PhD and MD in the Division of Biologic Sciences at the University of Chicago where she also began a residency in pathology. Her residency and fellowship was completed at Pennsylvania State University Medical Center. During this time, Dr. Unger developed a practical method of colorimetic in situ hybridization. This work led to interest in tissue localization of HPV and ultimately to her initial appointment to CDC in 1997 to pursue molecular pathology of HPV and CFS. Lauri E. Markowitz, Gui Liu, Susan Hariri, Martin Steinau, Eileen F. Dunne, Elizabeth R. Unger “Prevalence of HPV After Introduction of the Vaccination Program in the United States” Pediatrics, Published Online 19 February 2016. http://pediatrics.aappublications.org/content/early/2016/02/19/peds.2015-1968
-----------------------------------------
Original E-mail I sent:
sent: Tue 7/19/2016 8:27 PM
http://www.gardasil.com/hpv-and-your-child/what-is-hpv/
-----------------------------------------
Jun 23, 2016, 1:52 PM
Robyn Erland shared a link. (from facebook)
So we all know that Bill Reeves went to Panama and studied prostitutes with supposed HPV virus. It's what some of the HPV vaccine research is based on. Now he went there during the time the CFS money was misappropriated to other infectious disease areas. He was also head of the Herpes virus program as well as the CFS program. And we know Vernon and Unger were (Unger still is) also very much a part of the HPV vaccine sales currently being pushed starting with 9 year olds.
So here's the scoop. The NCI took Reeves research from the Panama prostitute studies and, These 2 NCI researchers work to develop a billion dollar HPV vaccine business for big Pharma!: Dr. Schiller and his co-PI Dr. Douglas Lowy led the initial development and characterization of the HPV prophylactic vaccines that ultimately became the commercial vaccines Cervarix and Gardasil.
And as I posted a couple weeks ago Fauci started an NCI/NIAID funded VACCINE RESEARCH PROGRAM. You see they get royalties off the technology that they give MERCK and Glasko-Smith Kline who make those vaccines. So do you see what's going on here?
Now the big problem is that children and young women have paid the price with their health, as many are instantly thrown into a chronic pain syndrome and several have died. And this research also comes from other countries who have little access to pap smears. See it's even debatable if HPV causes cervical cancer. And most is caught before any cancer happens. That's why only 3000 will die in the US ( not the millions they claim in this article) and a pap smear could save them. So starting with 9 year olds, it is they who are paying the price for inaccurate research coming from 3rd world countries and prostitute studies! This is about PROFIT not public Health!
Comes from the NCI/NIAID and the CDC: https://www.washingtonpost.com/national/health-science/cancer-doctors-leading-campaign-to-boost-use-of-hpv-vaccine/2016/06/19/1e5eb65a-2e8e-11e6-9de3-6e6e7a14000c_story.html
----------------------------------------------------
Jun 23, 2016, 1:52 PM
Robyn Erland shared a link. (from facebook)
About the Researcher who was given an NIAID CFS grant and is working with ex CDC employee Suzanne Vernon. Well Derya Unutmaz, M.D HIV immunologist came to Jackson labs from Norvartis Pharmaceuticals. They are a major company who dealt with XENOGRAFTING. Jackson labs also provide xenografts of mouse and human cells and provide the immunocompromised mice for the cancer research and they get funding from NCI.
Now take a look at these documents Xenotransplantation documents from Norvartis UK.See page 7 for the Norvartis name. Then see pages 18 and 19 where it talks about Risk assessment. See page 19 d) where it says "you may be aware of the fatality from the Simian Herpes B Virus of an American Lab worker from conjuctival contamination during weighing procedures.
Sent: Sunday, June 5, 2016 12:07 PM
Subject: HPV vax history - NIAID2007 vax Jordon report
Check out this 2007 Jordan Report from NIAID. Page 87 talks about NCI licensed the technology to Merck and Glaxo. So they base the 2 strains HPV 16and 18 on high risk groups and countries with little access to health care. These 2 researchers from NCI developed technology underlying the FDA-approved HPV vaccines. Dr. Douglas Lowy and Dr. John Schiller describe their quest for an HPV vaccine to aid in preventing cervical cancer at the National Institutes of Health (NIH) Intramural Researcher Program (IRP). More info on Dr. Lowy:
Dr. Lowy is being recognized for his key discoveries that led to development of the human papillomavirus (HPV) vaccine to prevent cancer. The vaccine developed by Dr. Lowy (in collaboration with Merck and GlaxoSmithKline), and approved by the FDA in 2006, was the first licensed vaccine to prevent cancer by guarding against the sexually transmitted infection that causes the disease.
So Dr. Lowy was involved with both these vaccines.
(Three vaccines are approved by the FDA to prevent HPV infection Merck did Gardasil and Glaxo-Smith Kline made Cervarix: Gardasil, Gardasil 9, and Cervarix. All three vaccines prevent infections with HPV types 16 and 18, two high-risk HPVs that cause about 70 percent of cervical cancers and an even higher percentage of some of the other HPV-associated cancers (9, 10). Gardasil also prevents infection with HPV types 6 and 11, which cause 90 percent of genital warts (17). Because Gardasil protects against infection with four HPV types, it is called a quadrivalent vaccine. Gardasil 9 prevents infection with the same four HPV types plus five additional high-risk HPV types (31, 33, 45, 52, and 58) and is therefore called a nonavalent, or 9-valent, vaccine. All three vaccines are given through a series of three injections into muscle tissue over a 6-month period.)
Human papillomavirus (HPV) is the name given to a group of viruses that includes more than 100 different strains. Almost every cervical cancer in the United States and abroad is caused by sexually transmitted infection with HPV. Two dominant strains of HPV, types 16 and 18, together cause 70 percent of new cases of cervical cancer. In 2006, a vaccine to prevent infection by these two HPV types was approved by the U.S. Food and Drug Administration (FDA). This vaccine, based primarily on technology developed by scientists from the National Cancer Institute’s (NCI) Center for Cancer Research, offers great hope for reducing the global burden of cervical cancer.
Dr. Lowy, who is involved in studies of both vaccines - See more at: http://www.curetoday.com/publications/cure/2006/special-issue2006/first-approved-hpv-vaccine-could-slash-number-of-cervical-cancers#sthash.0xFYfKLh.dpuf
Using molecular biology techniques, NCI scientists engineered a vaccine to prevent HPV infection. They demonstrated that the major HPV capsid protein by itself can self-assemble into non-infectious virus-like particles (VLPs) that are highly immunogenic. Immunization with these VLPs, which lack any infectious or oncogenic genetic material, stimulates production of large quantities of antibodies that prevent HPV virus infections in humans.
NCI licensed the technology to two pharmaceutical companies, Merck and GlaxoSmithKline (GSK), to develop HPV vaccines commercially. Both companies are running large-scale Phase III trials of their versions of an HPV vaccine. GSK’s targets the two most oncogenic HPV strains, 16 and 18. Merck’s vaccine also targets strains 16 and 18, as well as strains 6 and 11, which cause about 90 percent of genital warts. Phase II trials by both companies produced encourag Low-Risk and High-Risk HPVs. This chart shows the three groups of genital HPV strains. While the majority of infections with high-risk HPVs clear up on their own, a few can trigger cervical cancer over time. Courtesy of NCI ing results. The VLP vaccines were more than 90 percent effective at preventing infection with the virus that can lead to the development of premalignant cervical abnormalities. Studies to date have demonstrated that the vaccine prevents infection for up to four years after vaccination. Studies are under way to determine if a booster, in addition to the three initial intramuscular injections, will be necessary for long-term protection. Merck submitted an application for FDA approval and on June 8, 2006, Gardasil was approved as the first vaccine developed to prevent cervical cancer, precancerous genital lesions, and genital warts due to HPV types 6, 11, 16, and 18.
NCI’s involvement in optimizing HPV vaccine development continues. NCI scientists have developed the first high-throughput assay to enable HPV vaccine developers to monitor protective antibody responses long term, and test whether their new vaccines can induce potentially protective antibody responses against other strains of HPV.
In anticipation of FDA approval of HPV vaccines, the Gates Foundation announced in June 2005 that it would grant $12.9 million to the World Health Organization, the International Agency for Research on Cancer, Harvard University, and the Program for Appropriate Technology in Health to establish systems to ensure quality control in vaccine distribution, monitor the impact of different HPV vaccination strategies, and facilitate introduction of the vaccines worldwide.
Jordon Report - Accelerated Vaccines
https://www.niaid.nih.gov/sites/default/files/jordan2007.pdf
----------------------------------------------
Original E-mail I sent:
On May 22, 2016, at 1:46 PM
See the info below this first part for the pediatrics HPV stuff. Unger worked with Reeves and Vernon in CFS long ago
Posted: December 17, 2010
Elizabeth (Beth) Unger, PhD, MD, has been selected to serve as the Chief of the Chronic Viral Diseases Branch (CVDB) in the Division of High-Consequence Pathogens and Pathology (DHCPP), National Center for Emerging and Zoonotic Infectious Diseases (NCEZID), Centers for Disease Control and Prevention (CDC).
Dr. Unger has served as the Acting Chief of CVDB since January 2010 and has 13 years of experience in CVDB, where she has participated in the design and implementation of CFS research and HPV laboratory diagnostics.
During this time, she was co-author on 25 peer-reviewed manuscripts related to CFS, including the often-cited descriptions of the Wichita and Georgia population-based studies. In addition, Dr. Unger has been instrumental in efforts by WHO to establish an HPV LabNet and serves as lead of a WHO HPV Global Reference Laboratory.
She is co-author of 142 peer-reviewed publications and 24 book chapters and serves on the editorial board of six scientific journals. In 2008, for her HPV research accomplishments, she received the Health and Human Services (HHS) Career Achievement Award.
Dr. Unger received an undergraduate degree in Chemistry at Lebanon Valley College, Annville, PA. She then earned her PhD and MD in the Division of Biologic Sciences at the University of Chicago where she also began a residency in pathology. Her residency and fellowship was completed at Pennsylvania State University Medical Center. During this time, Dr. Unger developed a practical method of colorimetic in situ hybridization. This work led to interest in tissue localization of HPV and ultimately to her initial appointment to CDC in 1997 to pursue molecular pathology of HPV and CFS. Lauri E. Markowitz, Gui Liu, Susan Hariri, Martin Steinau, Eileen F. Dunne, Elizabeth R. Unger “Prevalence of HPV After Introduction of the Vaccination Program in the United States” Pediatrics, Published Online 19 February 2016. http://pediatrics.aappublications.org/content/early/2016/02/19/peds.2015-1968
-----------------------------------------
Original E-mail I sent:
sent: Tue 7/19/2016 8:27 PM
http://www.gardasil.com/hpv-and-your-child/what-is-hpv/
-----------------------------------------
Jun 23, 2016, 1:52 PM
Robyn Erland shared a link. (from facebook)
So we all know that Bill Reeves went to Panama and studied prostitutes with supposed HPV virus. It's what some of the HPV vaccine research is based on. Now he went there during the time the CFS money was misappropriated to other infectious disease areas. He was also head of the Herpes virus program as well as the CFS program. And we know Vernon and Unger were (Unger still is) also very much a part of the HPV vaccine sales currently being pushed starting with 9 year olds.
So here's the scoop. The NCI took Reeves research from the Panama prostitute studies and, These 2 NCI researchers work to develop a billion dollar HPV vaccine business for big Pharma!: Dr. Schiller and his co-PI Dr. Douglas Lowy led the initial development and characterization of the HPV prophylactic vaccines that ultimately became the commercial vaccines Cervarix and Gardasil.
And as I posted a couple weeks ago Fauci started an NCI/NIAID funded VACCINE RESEARCH PROGRAM. You see they get royalties off the technology that they give MERCK and Glasko-Smith Kline who make those vaccines. So do you see what's going on here?
Now the big problem is that children and young women have paid the price with their health, as many are instantly thrown into a chronic pain syndrome and several have died. And this research also comes from other countries who have little access to pap smears. See it's even debatable if HPV causes cervical cancer. And most is caught before any cancer happens. That's why only 3000 will die in the US ( not the millions they claim in this article) and a pap smear could save them. So starting with 9 year olds, it is they who are paying the price for inaccurate research coming from 3rd world countries and prostitute studies! This is about PROFIT not public Health!
Comes from the NCI/NIAID and the CDC: https://www.washingtonpost.com/national/health-science/cancer-doctors-leading-campaign-to-boost-use-of-hpv-vaccine/2016/06/19/1e5eb65a-2e8e-11e6-9de3-6e6e7a14000c_story.html
----------------------------------------------------
Jun 23, 2016, 1:52 PM
Robyn Erland shared a link. (from facebook)
About the Researcher who was given an NIAID CFS grant and is working with ex CDC employee Suzanne Vernon. Well Derya Unutmaz, M.D HIV immunologist came to Jackson labs from Norvartis Pharmaceuticals. They are a major company who dealt with XENOGRAFTING. Jackson labs also provide xenografts of mouse and human cells and provide the immunocompromised mice for the cancer research and they get funding from NCI.
Now take a look at these documents Xenotransplantation documents from Norvartis UK.See page 7 for the Norvartis name. Then see pages 18 and 19 where it talks about Risk assessment. See page 19 d) where it says "you may be aware of the fatality from the Simian Herpes B Virus of an American Lab worker from conjuctival contamination during weighing procedures.
So this American lab worker died from a monkey herpes b virus that splashed in their eye!
This was the danger of using animals in xenotransplantation, which also includes the used of MICE in xenografting for cancer research. And those mice carry infectious retroviruses and can recombine with other retroviruses to produce new infectious retroviruses.. This group in these papers tried shutting down xenotransplantation. Here is more on the documents they were able to eventually obtain from Norvartis: http://www.xenodiaries.org/docs.pdf#page=7&zoom=auto,-20,797
------------------------------------------------
Jun 15, 2016, 10:42 PM
Robyn Erland shared a link. (from facebook)
This is interesting from 2001. It's Beth Unger, Bill Reeves and FDA Advisory board member discussing HPV and how hard it is to diagnose, oh and how other animals get it too. Wonder how that came about. Could it be particles in the labs getting into cell lines too. And they discussed SmithKline's (sic) vaccine, LYMErix." and how it was giving children adverse reactions, see this members comment: (The FDA's decisive action is important to pull this from the product. Let me cover several sections that I believe are important. As you know, there has been great concern about the OspA vaccine having a cross-reactive effect to certain genetically vulnerable populations). Another member stated this: "And you ought to ask why Dr. Steere didn't come in and tell you why he is not getting the vaccination himself. Interesting, isn't it? He lives in Boston, I think, and I think he visits Cape Code I would assume.". My note: Oh and Dr. Allen Steere was a tuskeegee researcher by the way. Oh and this from the meeting: There are serious concerns from the FDA data on the protocol itself, and on how the data was reported.
https://web.archive.org/web/20021023190334/http://www.fda.gov/ohrms/dockets/ac/01/transcripts/3805t1.htm
-------------------------------------------
Jun 4, 2016, 11:21 PM
Robyn Erland shared a link. (from facebook)
So I posted about the NIH/NIAID/NCI Vaccine Research Center that was built and set up in 1999. Now this is funded by Fauci as it is housed under the NIAID and the National Cancer Institute. Now remember it was Harold Varmus who was instrumental as the NIH Director in 1999 to reinstate using animal retroviruses in research, namely cancer research which consists of xenografting animal and human tumor cells together. And remember that they found the mlv retroviruses in many of those xenograft cell lines in labs and in some non-xenografted cell lines just kept in with the xenograft ones. Because they became airborne.
Now this NIH Vaccine Research Center was originally set up as an AIDS Vaccine center. Now we have to ask why would they need a huge center to make ONE Aids vaccine in 2001? Well because they knew they planned to eventually use it for MANY vaccines because it's big business. And they are making new vaccines and technology. And we have to wonder why after 16 years there is still no AIDS vaccine given the fact tons of money has been poured into this center?
This center also gives 100's of scientists jobs. And they've been using contaminated retrovirus laced cell lines for decades! You really have to check out all this info and where your tax dollars go. We basically pay for the sickness and cancer they give us. They also started the ruling to vaccinate all children under 2. It's part of their goal. It was called the campaign "Every Child by Two." which the NIH implemented. But I don't think the 2 women who started the campaign realized people would be getting what comes in those vaccines. The retrovirual particles and all!
http://www.thebody.com/content/art6306.html
------------------------------------------------
Jun 4, 2016, 10:16 PM
Robyn Erland shared a link. (from facebook)
Look who the founders are for the NIH Vaccine Research center at the NIH:
"Right from the start, the VRC fashioned itself as a center for all of vaccinology, not just AIDS, explained two of the center’s founding influences, NIAID director Dr. Anthony Fauci and NCI director (and former NIH director) Dr. Harold Varmus. They made the case for a vaccine center to the Clinton administration in the mid-1990s."
https://nihrecord.nih.gov/newsletters/2011/04_29_2011/story1.htm
--------------------------------------------------
Jun 2, 2016, 12:59 PM
Robyn Erland shared a link. (from facebook)
So does everyone wonder who funded the 1986 Bill Reeves HPV Panama prostitute study that helped tie in 2 strains of HPV 16 and 18 from high risk groups. All this was done to help market the HPV vaccine onto 9 year olds, throwing some into instant a chronic pain ME permanent condition? Well it was the NIH and NCI who funded Reeves study. http://grantome.com/grant/NIH/R01-CA042042-04
---------------------------------------------------
Jun 2, 2016, 11:21 AM
Robyn Erland updated her status. (from facebook)
I stumbled across this today that all should read. The reason this is important is that it shows how the CFS funding was misapprpriated between 1995 and 1998. Now we know CDC employee of the herpesvirus branch and also CFS agency head Bill Reeves blew the whistle. But he was part of the misappropriated funds. Now his buddies and coworkers Suzanne Vernon and Elizabeth Unger have worked together in the HPV area since 1995 or before. They are on papers together. Beth Unger is actually still part of the HPV vaccine research as part of WHO and the CDC. Now did everyone know that Bill Reeves went to study HPV in Panama prostitutes and his research in 1997 was The basis for HPV vaccine technology? See the CFS money went to HPV, Borna, and enterovirus research instead of CFS research. So it was misappropriated. Now why is this important as it relates to HPV? Because Bill Reeves used hybrid technology that supposedly found HPV 16 and 18 in the the prostitutes which is claimed to cause cervical cancer. Now most who get HPV were getting the type that produces warts which is not cancerous. So why are 9 year olds being injected with something that has no purpose except in a high risk group in Panama?, and can also give them these children a chronic pain condition for life? We'll because it's for the money! Oh and for those on my page who don't know who Bill Reeves, Suzanne Vernon, and Beth Unger are They were all CDC employees who worked in HPV. Then Reeves was made head of the CFS program, Vernon came in and dusguised herself as a CFS advocate while helping to bury the pesky retroviruses in the blood supply and cell lines. Reeves died a few years ago and guess what they put Beth Unger in charge of the CFS CDC program, oh and Unger still works in the area of pushing HPV fraud data for producing even more HPV vaccines on the children. I'll post all the proof tomorrow with their papers. At least now we know where that money went. You will want to read this link until then. it's most revealing.
https://graham.main.nc.us/~bhammel/INS/jm19.html
----------------------------------------------
Jun 1, 2016, 12:04 AM
Robyn Erland shared a link. (from facebook)
While we're on the subject of cell lines ( some used for vaccines) Here is something that all should see again. This is one of the papers that because of the XMRV Science paper, it prompted agency heads to look for retroviruses in cell lines. So why is this important? Because in the paper where this picture comes from they found several mlv retroviruses in cell lines. Several were unidentified. Meaning they had no clue what mlv retrovirus it was because they had not been previously found yet.
So these are cancer "Xenografted" cell lines and some "Non-xenografted" cell lines that were kept in the same laboratory. Xenografting means the grafting of the mouse or mlv retrovirus together with human tumor cells. Now what they found was (because they were finding mlv's in the cells lines that shouldn't or previously had not been in the cell lines) Were that the xenografted cell lines cause the retoviruses in them to vertically transmit into other cell lines in the lab. And it was happening in both xenograft and non-xenograft lines. They also detemined in the paper that cell lines housed in other labs without these xenograft ones were clean of the mlv's.
Now the problem with this is that they never realized about this "transmitting of both endogenous retroviruses and infectious exogenous ones prior to 2011". And they have been housing the animal xenograft in with other cell lines some used for making vaccines and other biologicals for DECADES! And the manufacturing guidelines for vaccines allowed for mlv's in the finished products. That is not a good thing! http://www.frontiersin.org/files/Articles/55002/fonc-03-00156-HTML/image_m/fonc-03-00156-t001.jpg
---------------------------------------------
May 27, 2016, 12:20 PM
Robyn Erland shared a link. (from facebook)
http://finance.yahoo.com/news/officials-cover-dangers-hpv-vaccine-172411282.html?soc_src=mediacontentstory&soc_trk=fb
More vaccine misconduct news!
----------------------------------------------
Jan 19, 2016, 12:09 AM
E-mail I sent to specific researchers regarding HPV Vaccine they were not aware of:
Sent: Sunday, June 5, 2016 12:07 PM
Subject: HPV vax history - NIAID 2007 vax Jordon report
Check out this 2007 Jordan Report from NIAID. Page 87 talks about NCI licensed the technology to Merck and Glaxo. So they base the 2 strains HPV 16and 18 on high risk groups and countries with little access to health care. These 2 researchers from NCI developed technology underlying the FDA-approved HPV vaccines. Dr. Douglas Lowy and Dr. John Schiller describe their quest for an HPV vaccine to aid in preventing cervical cancer at the National Institutes of Health (NIH) Intramural Researcher Program (IRP). More info on Dr. Lowy:
Dr. Lowy is being recognized for his key discoveries that led to development of the human papillomavirus (HPV) vaccine to prevent cancer. The vaccine developed by Dr. Lowy (in collaboration with Merck and GlaxoSmithKline), and approved by the FDA in 2006, was the first licensed vaccine to prevent cancer by guarding against the sexually transmitted infection that causes the disease.
Dr. Lowy, who is involved in studies of both vaccines. (Three vaccines are approved by the FDA to prevent HPV infection Merck did Gardasil and Glaxo-Smith Kline made Cervarix: Gardasil, Gardasil 9, and Cervarix. All three vaccines prevent infections with HPV types 16 and 18, two high-risk HPVs that cause about 70 percent of cervical cancers and an even higher percentage of some of the other HPV-associated cancers (9, 10). Gardasil also prevents infection with HPV types 6 and 11, which cause 90 percent of genital warts (17). Because Gardasil protects against infection with four HPV types, it is called a quadrivalent vaccine. Gardasil 9 prevents infection with the same four HPV types plus five additional high-risk HPV types (31, 33, 45, 52, and 58) and is therefore called a nonavalent, or 9-valent, vaccine. All three vaccines are given through a series of three injections into muscle tissue over a 6-month period.)
Human papillomavirus (HPV) is the name given to a group of viruses that includes more than 100 different strains. Almost every cervical cancer in the United States and abroad is caused by sexually transmitted infection with HPV. Two dominant strains of HPV, types 16 and 18, together cause 70 percent of new cases of cervical cancer. In 2006, a vaccine to prevent infection by these two HPV types was approved by the U.S. Food and Drug Administration (FDA). This vaccine, based primarily on technology developed by scientists from the National Cancer Institute’s (NCI) Center for Cancer Research, offers great hope for reducing the global burden of cervical cancer.
See more at: http://www.curetoday.com/publications/cure/2006/special-issue2006/first-approved-hpv-vaccine-could-slash-number-of-cervical-cancers#sthash.0xFYfKLh.dpuf
Using molecular biology techniques, NCI scientists engineered a vaccine to prevent HPV infection. They demonstrated that the major HPV capsid protein by itself can self-assemble into non-infectious virus-like particles (VLPs) that are highly immunogenic. Immunization with these VLPs, which lack any infectious or oncogenic genetic material, stimulates production of large quantities of antibodies that prevent HPV virus infections in humans.
NCI licensed the technology to two pharmaceutical companies, Merck and GlaxoSmithKline (GSK), to develop HPV vaccines commercially. Both companies are running large-scale Phase III trials of their versions of an HPV vaccine. GSK’s targets the two most oncogenic HPV strains, 16 and 18. Merck’s vaccine also targets strains 16 and 18, as well as strains 6 and 11, which cause about 90 percent of genital warts. Phase II trials by both companies produced encourag Low-Risk and High-Risk HPVs. This chart shows the three groups of genital HPV strains. While the majority of infections with high-risk HPVs clear up on their own, a few can trigger cervical cancer over time. Courtesy of NCI ing results. The VLP vaccines were more than 90 percent effective at preventing infection with the virus that can lead to the development of premalignant cervical abnormalities. Studies to date have demonstrated that the vaccine prevents infection for up to four years after vaccination. Studies are under way to determine if a booster, in addition to the three initial intramuscular injections, will be necessary for long-term protection. Merck submitted an application for FDA approval and on June 8, 2006, Gardasil was approved as the first vaccine developed to prevent cervical cancer, precancerous genital lesions, and genital warts due to HPV types 6, 11, 16, and 18.
NCI’s involvement in optimizing HPV vaccine development continues. NCI scientists have developed the first high-throughput assay to enable HPV vaccine developers to monitor protective antibody responses long term, and test whether their new vaccines can induce potentially protective antibody responses against other strains of HPV.
In anticipation of FDA approval of HPV vaccines, the Gates Foundation announced in June 2005 that it would grant $12.9 million to the World Health Organization, the International Agency for Research on Cancer, Harvard University, and the Program for Appropriate Technology in Health to establish systems to ensure quality control in vaccine distribution, monitor the impact of different HPV vaccination strategies, and facilitate introduction of the vaccines worldwide.
-----------------------------------------------
Robyn Erland shared a link. (from facebook)
http://www.judicialwatch.org/blog/2017/03/govt-still-pushing-hpv-vaccine-kids-decade-jw-exposed-deadly-side-effects/?utm_source=SilverpopMailing&utm_medium=email&utm_campaign=Tipsheet+3-15-17+%281%29&utm_content
Govt. Still Pushing HPV Vaccine on Kids a Decade after JW Exposed Deadly Side Effects
The vaccine is called Gardasil and in the last ten years Judicial Watch has uncovered troves of government records documenting its harmful side effects. The vaccine was scandalously fast-tracked by the Food and Drug Administration (FDA) and was ardently promoted by the Obama administration as a miracle shot that can prevent certain strains of cervical cancer caused by Human Papillomavirus (HPV). Instead it’s been linked to thousands of debilitating side effects, according to the government’s own daunting statistics. This includes thousands of cases of paralysis, convulsions, blindness and dozens of deaths. Back in 2008, after receiving the first disturbing batch of records from the Centers for Disease Control and Prevention (CDC), Judicial Watch published a special report detailing Gardasil’s approval process, side effects, safety concerns and marketing practices. Undoubtedly, it illustrates a large-scale public health experiment.
http://www.judicialwatch.org/blog/2017/03/govt-still-pushing-hpv-vaccine-kids-decade-jw-exposed-deadly-side-effects/
Mar 15, 2017, 11:34 AM
---------------------------------------------------
Original E-mail I sent:
Sent: Monday, May 23, 2016 8:22 PM
Subject: NIH partially owns HPV Vax also Merck and Glaxo
Subject: NIH partially owns HPV Vax also Merck and Glaxo
NIH Technology Licensed to Merck for HPV Vaccine
A new cancer vaccine developed by Merck makes use of a novel disease prevention strategy to protect against cervical cancer. The vaccine is based on research conducted at the NIH. Cervical cancer is the second most common form of cancer deaths in women worldwide. Each year roughly 233,000 women die from cervical cancer. In the US, 9710 women are diagnosed annually and 3,700 die from it.
Gardasil®, the new Merck vaccine, as well as a new vaccine in development by GlaxoSmithKline (GSK), could dramatically reduce that number.
Unlike many forms of cancer, cervical cancer is not strongly associated with a genetic predisposition. Rather it is attributed to infection by Human Papilloma Virus (HPV). HPV is associated with almost all cases of cervical cancer. HPV is a highly prevalent sexually transmitted disease (STD) and is the most common STD in the US. By age 50 approximately 80% of females have acquired the virus. HPV also causes benign genital warts. There are approximately 32 million cases of genital warts each year. Currently there are no effective therapeutic interventions for HPV infection. A pap smear can detect HPV induced pre-cancerous lesions which can then be surgically removed. However routine screening opportunities are not as affordable for women in poorer countries. As a result, the mortality rate from cervical cancer is much higher in these countries.
There are over 100 strains of HPV, many of which exhibit no symptoms and clear up on their own. But some strains are cause for particular concern, especially HPV16 and HPV18, which cause approximately 70% of cervical cancer world wide. HPV6 and HPV11, although generally considered to be nononcogenic, cause approximately 90% of genital warts. Gardasil® prevents infection against these four forms of HPV, in effect; preventing the majority of HPV related illnesses.
Gardasil®, the new Merck vaccine, as well as a new vaccine in development by GlaxoSmithKline (GSK), could dramatically reduce that number.
Unlike many forms of cancer, cervical cancer is not strongly associated with a genetic predisposition. Rather it is attributed to infection by Human Papilloma Virus (HPV). HPV is associated with almost all cases of cervical cancer. HPV is a highly prevalent sexually transmitted disease (STD) and is the most common STD in the US. By age 50 approximately 80% of females have acquired the virus. HPV also causes benign genital warts. There are approximately 32 million cases of genital warts each year. Currently there are no effective therapeutic interventions for HPV infection. A pap smear can detect HPV induced pre-cancerous lesions which can then be surgically removed. However routine screening opportunities are not as affordable for women in poorer countries. As a result, the mortality rate from cervical cancer is much higher in these countries.
There are over 100 strains of HPV, many of which exhibit no symptoms and clear up on their own. But some strains are cause for particular concern, especially HPV16 and HPV18, which cause approximately 70% of cervical cancer world wide. HPV6 and HPV11, although generally considered to be nononcogenic, cause approximately 90% of genital warts. Gardasil® prevents infection against these four forms of HPV, in effect; preventing the majority of HPV related illnesses.
The underlying technology for the vaccine originated in the laboratories of Drs. John Schiller and Douglas Lowy of the NIH National Cancer Institute. Drs. Schiller and Lowy commenced their research on the molecular biology of HPV nearly 20 years ago. Among their numerous findings, they discovered that the major outer coat protein of the virus, called L1, could self assemble into non-infectious virus-like particles (VLPs) that closely resemble the native outer shell of the actual virus.
The principle behind the vaccine is that exposure to VLPs triggers the immune system to produce protective antibodies. If an individual is exposed to HPV after receiving the vaccine, the immune system already contains the antibodies necessary to prevent virus infection. The antibodies primarily function by preventing the virus from binding to the cell which is necessary in order for the virus to reproduce and thrive.
The catch is that for induction of HPV neutralizing antibodies the L1 must be in the same conformation as in the intact virus. Unlike some other viral vaccines, inactivated virus produced in cultured cells was not a viable option because the viruses could not be produced in sufficient quantities in vitro. Also, the inactivated virions would still contain the viral oncogenes, which would preclude use in healthy young people, the primary target population. Schiller and Lowy demonstrated that large quantities of VLPs could be produced in insect cells infected with L1 recombinant baculovirus. Critically, they also showed in animal models that the L1 VLPs were able to induce high titers of neutralizing antibodies, comparable to those induced by authentic virions. Furthermore, they and their colleagues demonstrated that L1 VLP vaccination could protect animals from experimental challenge with high dose virus of the corresponding animal papillomavirus types and that human and animal papillomavirus L1 behaved similarly in the ability to assemble into VLP.
Working with the NCI technology transfer office, the NIH Office of Technology Transfer (OTT) oversaw the patenting of the VLPs. OTT then sought a suitable company with the necessary resources to formulate the vaccine and to conduct clinical trials. The technology was licensed to Merck, the maker of Gardasil®. In October 2005 Merck announced the results of it clinical trials. It was one of the most successful vaccine clinical trials ever. The phase II and phase III studies evaluated the effects of Gardasil® on 20,541 women between the ages of 16 and 26. The women were followed for up to 5 years. Remarkably, none of the women receiving Gardasil® developed precancerous cervical lesions caused by the HPV types in the vaccine. Gardasil® also had a 99% efficacy in preventing genital warts by the types targeted by the vaccine. Moreover, there is evidence that Gardasil® is effective at treatment of preexisting HPV infection. Merck applied for priority FDA review for the vaccine in December of 2005. GlaxoSmithKline, another licensee of the NIH VLP technology, is conducting efficacy trials of a VLP vaccine targeting HPV16 and HPV18. GSK applied for regulatory approval in Europe in March 2006, and is expected to apply for US FDA approval by the end of 2006.
On June 8th 2006, the FDA gave its final approval for Gardasil®. Gardasil® is currently approved for females ages 9 to 26. The vaccine is administered 3 times over a period of 6 months. Although not currently recommended for males, the FDA may in the future approve such use.
Merck is developing a patient assistance program for adults who are uninsured or who cannot afford the vaccine. Merck is seeking approval for Gardasil® in other countries around the world and is working with the global nonprofit health group PATH, with support from the Bill and Melinda Gates Foundation, to explore opportunities for distributing the vaccine in developing countries (see the full story).
Gardasil® marks a tremendous step forward in the prevention of STDs and cancer. Most treatments in the field of cancer aim to cure the disease, but this one is designed to prevent it. It is not only an achievement for cervical cancer but is a remarkable advance in the field of cancer vaccines and an extraordinary proof of principle. According to NCI Acting Director John E. Niederhuber, M.D., “This vaccine opens a new era in cancer prevention.” Women who receive Gardasil® will still need to receive routine screenings for cervical cancer as protection is strain restricted and 30% of cervical cancer cases are attributed to other HPV strains. There are currently over 100 cancer vaccines being developed by drug companies, although few are likely to be as efficacious as Gardasil®. The majority are not preventative like Gardasil® but, instead, help to boost the immune system of individuals who have already developed the disease. Hopefully, Gardasil® will pave the way for the development of other preventative cancer vaccines.
-----------------------------------------------
Robyn Erland copyright for my wording - This is from 2006. This means they were planning in 2006 to make up sales from the loss of sales and lawsuits that came from Vioxx. According to what others are reporting there are e-mails where Merck was letting the shareholders know that the HPV vaccines will more than make up fo the sales and lawsuit losses. Since there are no liability for harms from vaccines there is no worry about them being sued for harms and deaths of children from the HPV vaccines. Now we can see why they need to remove all exemptions from all vaccines. It's always about the money and their need for making clients for profit! From the 2006 article below:
"There might be enough good news to balance out the bad. Merck's 2006 gains have been driven by pipeline break-throughs with the cancer vaccine Gardasil.
But help is on the way. Merck recently received approval from the Food and Drug Administration for two vaccines - Gardasil, to prevent the sexually-transmitted virus that causes most cases of cervical cancer, and Zostavax, for the prevention shingles - as well as the diabetes drug Januvia. Analysts project comparatively modest annual sales of $300 million for Zostavax, but $1 billion for Januvia and up to $4 billion for Gardasil.
"We have high expectations for Gardasil," wrote Tim Anderson of Prudential Equity Group in an analyst's note, where he said vaccine sales could be fueled by routine vaccination in girls as young as 11 and 12. Anderson projects annual sales of $3.2 billion by 2010.
But even with these new drugs, Merck will have to scramble for more blockbusters to fill the impending sales gap while maintaining enough growth to keep investors happy.
"The big thing that's really holding it back is generic competition," said Rauch, noting that the company will have a difficult time keeping its pledge of double-digit growth, considering that half its revenue is disappearing between 2006 and 2012. "That's a lot of revenue you have to come with."
Rauch does not own shares of Merck stock but A.G. Edwards does have investments in the company. Anderson, or someone in his team or family, owns shares of Pfizer.
Related: Merck's dance with the religious right. Here's the article with link:
Merck and the Vioxx rut
No. 2 U.S. drugmaker works to balance legal fights, patent loss with strong pipeline.
By Aaron Smith, CNNMoney.com staff writer
July 4 2006: 9:19 AM EDT
NEW YORK (CNNMoney.com) -- Merck's stock price is starting to climb out of its hole this year, but the drug giant still faces a long uphill climb fraught with obstacles if it ever plans to get to its pre-Vioxx scandal levels.
Merck's (up $0.19 to $36.62, Charts) stock price gained more than 14 percent year-to-date through June 30, far outpacing the gains of drug industry as a whole and the S&P 500, which each rose 1.8 percent. Compare this to the market leader Pfizer (up $0.11 to $23.58, Charts), which has seen its price climb less than 1 percent year-to-date.

Merck's gain isn't too shabby, considering the company's stock plunged nearly 27 percent on its Day of Infamy -- Sept. 30, 2004. That's the day America's no. 2 drugmaker pulled Vioxx, an arthritis painkiller, off the market, following a study that linked the drug to increased risks of heart attack and stroke. This has since been a major concern for the company, which not only lost $2.5 billion in annual sales but now faces about 11,500 Vioxx-related lawsuits.
But despite Merck's impressive stock price gain this year, the price is still 19 percent below its level on Sept. 29, 2004 - the day before the word "Vioxx" became synonymous with "lawsuit."
There might be enough good news to balance out the bad. Merck's 2006 gains have been driven by pipeline break-throughs with the cancer vaccine Gardasil and the diabetes drug Januvia, as well as a strong dividend yield of 4.2 percent, said Al Rauch, analyst for A.G. Edwards & Sons.
"You buy good companies when they're having a tough time, and with these dividend yields you get paid while you wait," said Rauch.
But Rauch, who rates Merck a "neutral," said the company faces serious obstacles going forward, including the Vioxx-related lawsuits and a slew of patent expirations that are evaporating billions of dollars in annual revenue.
Merck bid adieu on June 23 to its patent for cholesterol-cutting drug Zocor, which totaled $4.4 billion in 2005 sales. This opens the drug up to generic competition, resulting in plummeting sales. But the company plans to curb the ensuing plunge with a partnership. Merck and Schering-Plough (up $0.14 to $19.17, Charts) have combined Zocor with the Schering drug Zetia for the drug-combo Vytorin that totaled $2.4 billion in 2005 sales.
But Rauch said that Merck faces serious challenges in its patent expirations on other top-selling drugs: Folsom, the $3.2 billion treatment for post-menopausal osteoporosis, is going off-patent in 2008; Cozaar, the anti-hyperintensive drug worth $3 billion in annual sales when grouped with Hyzaar, off-patent in 2010, and Singulair, the $3 billion treatment for chronic asthma, off-patent in 2012.
But help is on the way. Merck recently received approval from the Food and Drug Administration for two vaccines - Gardasil, to prevent the sexually-transmitted virus that causes most cases of cervical cancer, and Zostavax, for the prevention shingles - as well as the diabetes drug Januvia. Analysts project comparatively modest annual sales of $300 million for Zostavax, but $1 billion for Januvia and up to $4 billion for Gardasil.
"We have high expectations for Gardasil," wrote Tim Anderson of Prudential Equity Group in an analyst's note, where he said vaccine sales could be fueled by routine vaccination in girls as young as 11 and 12. Anderson projects annual sales of $3.2 billion by 2010.
But even with these new drugs, Merck will have to scramble for more blockbusters to fill the impending sales gap while maintaining enough growth to keep investors happy.
"The big thing that's really holding it back is generic competition," said Rauch, noting that the company will have a difficult time keeping its pledge of double-digit growth, considering that half its revenue is disappearing between 2006 and 2012. "That's a lot of revenue you have to come with."
Rauch does not own shares of Merck stock but A.G. Edwards does have investments in the company. Anderson, or someone in his team or family, owns shares of Pfizer. https://money.cnn.com/2006/07/03/news/companies/merck/index.htm?fbclid=IwAR2Yue35H-pT0QfB-Zx5i_ujY0yDAqwxEQ4CSAK8ZMmN0-iJ3slV0VhFe0s
Related: Merck's dance with the religious right
 see below
see belowMerck's dance with the religious right
Drug giant close to approval for controversial anti-cancer vaccine for youngsters.
By Aaron Smith, CNNMoney.com staff writer
May 16, 2006: 2:58 PM EDT
NEW YORK (CNNMoney.com) - Merck needs a hit, and it just might be on the verge of getting one, thanks to some delicate footwork with the religious right.
Merck is eagerly awaiting news from the Food and Drug Administration, which is due to make a decision on two key experimental vaccines in the next few weeks. One of those is Gardasil, a controversial vaccine for the prevention of cervical cancer.
If approved Gardasil could be a multi-billion blockbuster for Merck. However the vaccine is used to inoculate young girls from contracting a sexually transmitted cancer virus later in life. Conservative religious groups worry that use of the vaccine may send the wrong message about premarital sex.
Through a carefully orchestrated "informational" campaign, Merck has managed to overcome that resistance. And now it may be about to win the government's okay as well.
An advisory committee for the FDA will vote on greenlighting Gardasil on May 18. A "yes" vote will clear the way for ultimate FDA approval, since the agency usually follows the lead of its panels. The FDA is scheduled to complete its review of Gardasil on June 8.
The experimental vaccine is backed by strong clinical data and has been hailed as a bright light for Merck (up $0.60 to $35.29, Research), a drug giant that is losing billions of dollars in annual sales to impending patent expirations, as well as the withdrawal of its blockbuster Vioxx.
"It shows that there's life after Vioxx," said Les Funtleyder, analyst for Miller Tabak, referring to the vaccine.
About Gardasil
Gardasil is most effective, as a preventative, when used in children. The vaccine has been tested in boys and girls as young as 10, with the intention of inoculating them years before they become sexually active.
The data from Gardasil late-stage studies has been strong. Gardasil has shown 100 percent efficacy in preventing the sexually transmitted human papillomavirus, which causes 70 percent of cervical cancer cases, according to Merck. This type of cancer kills nearly 4,000 women in the U.S. annually and nearly 300,000 worldwide, according to the National Cervical Cancer Coalition.
Gardasil has also shown 100 percent efficacy in preventing the sexually-transmitted viruses that cause 90 percent of vaginal and vulvar lesions in young women, including genital warts, according to Merck.
If the FDA approves Gardasil, it would help fill part of the sales vacuum left by Vioxx, an arthritis painkiller that Merck pulled off the market in 2004 after a study showed an increased the risk of heart attacks and strokes. Not only did this erase $2.5 billion in annual sales, but about 11,500 lawsuits have been filed against Merck by former patients and their families.
Analysts put a wide range on the potential Vioxx fallout. While Barbara Ryan of Deutsche Bank North America projects that damages could total $30 billion for Merck, David Moskowitz of Friedman, Billings, Friedman projects $50 billion, the highest projection in the industry.
In addition to the Vioxx troubles, Merck's patent on its top-selling drug, the cholesterol-cutting Zocor, expires on June 23, taking away $4.4 billion in annual sales.
Gardasil sales could reach $1.6 billion annually by 2009, said Ryan of Deutsche Bank North America. Jami Rubin, analyst for J.P. Morgan, projects annual sales of $2 billion.
All about the age
But Funtleyder of Miller Tabak said sales are dependant on whether the vaccine is approved for all ages.
"What's the age range?" said Funtleyder. "Are they going to make people in the religious right freak out?"
Girls as young as 11 could be approved to use the vaccine. But the idea of children that young being inoculated against a sexually transmitted disease is upsetting to many parents and parental groups.
So Merck's recent educational campaign has focused on prevention of HPV and cervical cancer, and de-emphasized sexuality.
"Merck continues to work with all organizations to understand diverse positions and make people feel comfortable about broad use of Gardasil," said Merck spokeswoman Kelley Dougherty.
And that has apparently been a winning strategy. Dougherty the company has managed to win growing support for Gardasil over the last year.
"How could anyone be against vaccination against a common virus that causes cervical cancer?" asked Ryan. "I think, in that way, [Merck] is successfully walking down the path that will minimize complications along those lines."
Focus on the Family and the Family Research Council, both faith-based conservative policy organizations, recently have spoken in support of HPV vaccines from Merck and GlaxoSmithKline because of their life-saving potential. But the organizations still promote abstinence before marriage as the best way to prevent infection.
"The HPV vaccine does not, in any circumstances, negate or substitute God's plan for sexuality, which is sexual abstinence until marriage and sexual faithfulness within marriage," said Focus on the Family spokeswoman Linda Klepacki in a statement on the organization's Web site.
J.P. Morgan's Rubin observed the FDA will be closely watched to make sure it doesn't reject Gardasil based on morality instead of science, as the agency is accused of doing in its failure to approve birth control pill Plan B for over-the-counter availability. The FDA said it did not approve Plan B for OTC use because there was not enough data involving girls under the age of 16, even though its advisory committee had recommended approval.
"I think the FDA's failure to approve Plan B [as an over-the-counter drug] despite the FDA advisory committee's support on this probably backfired on them," said Rubin.
Funtleyder of Miller Tabak said that Gardasil won't be as politically difficult to get past the FDA as Plan B, because Plan B is a birth control drug and Gardasil is not.
"Certainly the same political forces that were in operation then are in operation now," said Funtleyder. "But [Gardasil] is a different product. [Plan B] was closer to contraception [than Gardasil.]"
Merck's Gardasil could eventually face competition from GlaxoSmithKline's (up $1.20 to $58.28, Research) Cervarix, which is also being tested for the prevention of human papillomavirus but is at least one year behind Merck's drug. Rubin of J.P. Morgan projects that Cervarix sales could reach $1.6 billion annually.
Zostavax, the shingles vaccine
In another positive development for Merck, although not as big dollar-wise, the FDA is expected to make a decision on Zostavax, Merck's shingles vaccine, on May 25.
Annual sales projections for Zostavax tend to peak at around $200 million, a drop in the bucket compared to the company's $22 billion sales total for 2005.
Zostavax was developed as a vaccine against shingles, a blistering rash caused by the latent varicella virus, which also causes chicken pox. Merck published the findings of late-stage studies last year in The New England Journal of Medicine, showing that the vaccine reduced the incidence of shingles by 51 percent. Merck also said that, in those not successfully inoculated, the vaccine reduced pain and discomfort in shingles patients by 61 percent and reduced persistent nerve pain, the most common symptom, by 67 percent.
There seems to be little doubt that Zostavax will be approved by the FDA. Back in December, an FDA advisory committee recommended approval of Zostavax. On its Web site, the National Institutes of Health seemed to give Zostavax an endorsement, because if approved by the FDA it "has the potential to prevent hundreds of thousands of cases of shingles in the U.S. in a single year."
The analysts interviewed for this story do not own shares of Merck stock. https://money.cnn.com/2006/05/15/news/economy/merck/index.htm
To read about Merck's first quarter earnings, click here. or see below
Merck's strong quarter boosts year forecast
No. 2 drugmaker tops 1Q estimates on strong sales of cholesterol drug; cost-cutting credited for profit strength.
By Aaron Smith, CNNMoney.com staff writer
April 20, 2006: 12:55 PM EDT
NEW YORK (CNNMoney.com) - Merck reported strong first-quarter profit Thursday, beating consensus projections on a slight increase in sales, and prompting the drugmaker to ramp up its earnings projection for the full year despite the imminent patent loss of its top-selling product, Zocor.
Shares of Merck (up $0.69 to $35.09, Research) rose as much as 2.5 percent in New York Stock Exchange trading.
Merck reported net profit of $1.52 billion, or 69 cents per share, up from $1.37 billion last year, or 62 cents a share. Excluding a 9-cent-a-share charge related to its cost-cutting, Merck reported earnings per share of 78 cents, beating First Call consensus projections of 72 cents.
The second-biggest drugmaker in the U.S. said sales increased 1 percent to $5.41 billion.
"We're very confident," said chief executive officer Dick Clark in a conference call with analysts. "No miracles have to happen here. It's just focus on the business and get your results. Obviously there's a long way to go, but I think we're on the right path."
The company, based in Whitehouse Station, N.J., said the strong profit was partly driven by sales from Zocor, a cholesterol-cutting blockbuster, as well as the asthma drug Singulair. Merck also attributed the earnings increase to its $5 billion belt-tightening plan to cut up to 7,000 jobs and close or sell five drug making plants.
The strong quarter prompted Merck to increase its full-year 2006 guidance to a range of $2.32 to $2.40 earnings per share, from its previously projected range of $2.28 to $2.36.
Merck's chief financial officer Judy Lewent said during the analyst call that the guidance was ramped up "to reflect that we had a strong first quarter."
The company increased projections in spite of the fact that Zocor, its No. 1 seller with $4.4 billion in 2005 revenue, is losing patent protection June 23, which is expected to trigger a plunge in sales. In the first quarter, Zocor sales rose 13 percent to $1 billion, possibly fueled by new prescriptions in anticipation of the patent loss, which would mean cheaper prices for patients when they switch to generic versions of the drug.
Merck announced that the tally of lawsuits from former patients of Vioxx, an arthritis painkiller that was pulled off the market in 2004 after a study showed increased risk of heart attack and strokes, has increased to 11,500. But Merck did not increase the fund set aside for its legal defense, which was last reported at $690 million. This fund does not cover potential damages to the company.
So far, Merck has lost one case and won two, and there was a split verdict in the most recent case.
Cost-cutting key driver in strong earnings
"I suspect they're raising earnings projections on better cost control," said Les Funtleyder, analyst for Miller Tabak, referring to Merck's multi-billion dollar cost-cutting plan. "Also, I got the sense that they think their new product launches are going to be better than we thought." Funtleyder rates the company a "buy" with a $40 price target.
Merck is awaiting the Food and Drug Administration's decision on Gardasil, its vaccine to prevent a virus that causes cervical cancer. The FDA has given the drug priority review status, generally a very good sign for potential approval, and the agency's decision is tentatively scheduled for June 8.
Analysts have been bullish on Gardasil, a potential blockbuster that has enjoyed strong data in clinical studies. Last year, the company unveiled two studies: one showing 100 percent efficacy in preventing the sexually transmitted human papillomavirus, which causes 70 percent of cervical cancer cases, and another showing 100 percent efficacy in preventing the sexually transmitted virus that causes 90 percent of vaginal lesions in young women, including genital warts.
CEO Clark also mentioned the recent FDA approval of Rotateq, a vaccine for rotavirus in children and babies, and the filing of Januvia, a diabetes treatment, as products that will drive Merck sales going forward.
The company also hopes to recover some of the impending Zocor sales vacuum with the cholesterol drug Vytorin, which combines Zocor with Schering-Plough's (up $0.42 to $19.31, Research) Zetia. Launched in 2004, Vytorin sales totaled $2.4 billion in 2005 sales.
Barbara Ryan of Deutsche Bank North America said in a note that Merck's biggest challenge, the Vioxx liability, has already been baked into the stock price, which has been discounted for $30 billion worth of possible damages.
"We believe Merck has put in place an aggressive, but achievable strategic plan, and with a new management team that is motivated and determined to execute, with a new sense of urgency and accountability," wrote Ryan, who rates Merck a "buy" with a price target of $38.
David Moskowitz, analyst for Friedman, Billings, Ramsey, has projected the highest Vioxx damage estimate, at $50 billion.
--
To read about Big Pharma v. biotechs in year-to-date stock performance, click here.
The analysts interview for this story do not own Merck stock, but Deutsche Bank North America does seek business with them.
---------------------------------------------
Robyn Erland copyright my wording - Here's and another posting I made on gardasil profits in 2016:
Robyn Erland
Mar 28, 2016 11:52 AM
who.int
Check this out. It's the WHO Global Vaccine Market information. And here are some of the highlights from it:
RAPID GROWTH and CHANGING STATUS
Tripled in value from USD 5 Billion in 2000 to almost USD 24 Billion in 2013
Global market projected to rise to USD 100 Billion by 2025
More than 120 new products in the development pipeline
Vaccines: becoming an engine for the pharmaceutical industry
hanging status of the vaccines within the pharmaceutical industry
New business model for vaccines is emerging?
Newer and more expensive vaccines are coming into the market faster than ever before
Vaccine development: increasing investment
2010 sales (US$)
Prevnar
-
13 (Pfizer) valent pnenumococcal
conjugate vaccine
$2.4 billion
Proquad (Merck/Sanofi-Aventis)
Measles - mumps -rubella and
varicella combination vaccine
(MMR - V)
$1.4 billion
Gardasil (Merck)
HPV
$1.35 billion
Prevnar (Pfizer)
valent pnenumococcal conjugate
vaccine
$1.2 billion
Fluzone (Sanofi Pasteur)
Influenza (seasonal and H1N1 strains)
$1.2 billion
Infanrix and Pediarix) (GSK)
Infanrix = DTaP
Pediarix = DTap - HepB - IPV
(combination DPT - based vaccines
with acellular pertussis)
$1.2 billion
You all really should take a look at these profits. And with zero liability for any harm done to anyone, it is a win win for the pharmaceutical manufacturers once the law was put in saying they could never be sued. Even for deaths they cause. It's also no wonder they have made even infants their newest clients. Zero liability with huge profit going into their fat pockets. And who pays the price for injuries or the diseases that come with their retrovirus lab recombinations that wound up in cell lines for decades? We do!!!
https://www.who.int/influenza_vaccines_plan/resources/session_10_kaddar.pdf?fbclid=IwAR0JzZWjw0ckcTf878KJ7n91mizsvL4iqvZKJyOzHwK-R9yisCpNBkfEt0I
But Funtleyder of Miller Tabak said sales are dependant on whether the vaccine is approved for all ages.
"What's the age range?" said Funtleyder. "Are they going to make people in the religious right freak out?"
Girls as young as 11 could be approved to use the vaccine. But the idea of children that young being inoculated against a sexually transmitted disease is upsetting to many parents and parental groups.
So Merck's recent educational campaign has focused on prevention of HPV and cervical cancer, and de-emphasized sexuality.
"Merck continues to work with all organizations to understand diverse positions and make people feel comfortable about broad use of Gardasil," said Merck spokeswoman Kelley Dougherty.
And that has apparently been a winning strategy. Dougherty the company has managed to win growing support for Gardasil over the last year.
"How could anyone be against vaccination against a common virus that causes cervical cancer?" asked Ryan. "I think, in that way, [Merck] is successfully walking down the path that will minimize complications along those lines."
Focus on the Family and the Family Research Council, both faith-based conservative policy organizations, recently have spoken in support of HPV vaccines from Merck and GlaxoSmithKline because of their life-saving potential. But the organizations still promote abstinence before marriage as the best way to prevent infection.
"The HPV vaccine does not, in any circumstances, negate or substitute God's plan for sexuality, which is sexual abstinence until marriage and sexual faithfulness within marriage," said Focus on the Family spokeswoman Linda Klepacki in a statement on the organization's Web site.
J.P. Morgan's Rubin observed the FDA will be closely watched to make sure it doesn't reject Gardasil based on morality instead of science, as the agency is accused of doing in its failure to approve birth control pill Plan B for over-the-counter availability. The FDA said it did not approve Plan B for OTC use because there was not enough data involving girls under the age of 16, even though its advisory committee had recommended approval.
"I think the FDA's failure to approve Plan B [as an over-the-counter drug] despite the FDA advisory committee's support on this probably backfired on them," said Rubin.
Funtleyder of Miller Tabak said that Gardasil won't be as politically difficult to get past the FDA as Plan B, because Plan B is a birth control drug and Gardasil is not.
"Certainly the same political forces that were in operation then are in operation now," said Funtleyder. "But [Gardasil] is a different product. [Plan B] was closer to contraception [than Gardasil.]"
Merck's Gardasil could eventually face competition from GlaxoSmithKline's (up $1.20 to $58.28, Research) Cervarix, which is also being tested for the prevention of human papillomavirus but is at least one year behind Merck's drug. Rubin of J.P. Morgan projects that Cervarix sales could reach $1.6 billion annually.
Zostavax, the shingles vaccine
In another positive development for Merck, although not as big dollar-wise, the FDA is expected to make a decision on Zostavax, Merck's shingles vaccine, on May 25.
Annual sales projections for Zostavax tend to peak at around $200 million, a drop in the bucket compared to the company's $22 billion sales total for 2005.
Zostavax was developed as a vaccine against shingles, a blistering rash caused by the latent varicella virus, which also causes chicken pox. Merck published the findings of late-stage studies last year in The New England Journal of Medicine, showing that the vaccine reduced the incidence of shingles by 51 percent. Merck also said that, in those not successfully inoculated, the vaccine reduced pain and discomfort in shingles patients by 61 percent and reduced persistent nerve pain, the most common symptom, by 67 percent.
There seems to be little doubt that Zostavax will be approved by the FDA. Back in December, an FDA advisory committee recommended approval of Zostavax. On its Web site, the National Institutes of Health seemed to give Zostavax an endorsement, because if approved by the FDA it "has the potential to prevent hundreds of thousands of cases of shingles in the U.S. in a single year."
The analysts interviewed for this story do not own shares of Merck stock. https://money.cnn.com/2006/05/15/news/economy/merck/index.htm
To read about Merck's first quarter earnings, click here.
or see belowMerck's strong quarter boosts year forecast
No. 2 drugmaker tops 1Q estimates on strong sales of cholesterol drug; cost-cutting credited for profit strength.
By Aaron Smith, CNNMoney.com staff writer
April 20, 2006: 12:55 PM EDT
NEW YORK (CNNMoney.com) - Merck reported strong first-quarter profit Thursday, beating consensus projections on a slight increase in sales, and prompting the drugmaker to ramp up its earnings projection for the full year despite the imminent patent loss of its top-selling product, Zocor.
Shares of Merck (up $0.69 to $35.09, Research) rose as much as 2.5 percent in New York Stock Exchange trading.
Merck reported net profit of $1.52 billion, or 69 cents per share, up from $1.37 billion last year, or 62 cents a share. Excluding a 9-cent-a-share charge related to its cost-cutting, Merck reported earnings per share of 78 cents, beating First Call consensus projections of 72 cents.
The second-biggest drugmaker in the U.S. said sales increased 1 percent to $5.41 billion.
"We're very confident," said chief executive officer Dick Clark in a conference call with analysts. "No miracles have to happen here. It's just focus on the business and get your results. Obviously there's a long way to go, but I think we're on the right path."
The company, based in Whitehouse Station, N.J., said the strong profit was partly driven by sales from Zocor, a cholesterol-cutting blockbuster, as well as the asthma drug Singulair. Merck also attributed the earnings increase to its $5 billion belt-tightening plan to cut up to 7,000 jobs and close or sell five drug making plants.
The strong quarter prompted Merck to increase its full-year 2006 guidance to a range of $2.32 to $2.40 earnings per share, from its previously projected range of $2.28 to $2.36.
Merck's chief financial officer Judy Lewent said during the analyst call that the guidance was ramped up "to reflect that we had a strong first quarter."
The company increased projections in spite of the fact that Zocor, its No. 1 seller with $4.4 billion in 2005 revenue, is losing patent protection June 23, which is expected to trigger a plunge in sales. In the first quarter, Zocor sales rose 13 percent to $1 billion, possibly fueled by new prescriptions in anticipation of the patent loss, which would mean cheaper prices for patients when they switch to generic versions of the drug.
Merck announced that the tally of lawsuits from former patients of Vioxx, an arthritis painkiller that was pulled off the market in 2004 after a study showed increased risk of heart attack and strokes, has increased to 11,500. But Merck did not increase the fund set aside for its legal defense, which was last reported at $690 million. This fund does not cover potential damages to the company.
So far, Merck has lost one case and won two, and there was a split verdict in the most recent case.
Cost-cutting key driver in strong earnings
"I suspect they're raising earnings projections on better cost control," said Les Funtleyder, analyst for Miller Tabak, referring to Merck's multi-billion dollar cost-cutting plan. "Also, I got the sense that they think their new product launches are going to be better than we thought." Funtleyder rates the company a "buy" with a $40 price target.
Merck is awaiting the Food and Drug Administration's decision on Gardasil, its vaccine to prevent a virus that causes cervical cancer. The FDA has given the drug priority review status, generally a very good sign for potential approval, and the agency's decision is tentatively scheduled for June 8.
Analysts have been bullish on Gardasil, a potential blockbuster that has enjoyed strong data in clinical studies. Last year, the company unveiled two studies: one showing 100 percent efficacy in preventing the sexually transmitted human papillomavirus, which causes 70 percent of cervical cancer cases, and another showing 100 percent efficacy in preventing the sexually transmitted virus that causes 90 percent of vaginal lesions in young women, including genital warts.
CEO Clark also mentioned the recent FDA approval of Rotateq, a vaccine for rotavirus in children and babies, and the filing of Januvia, a diabetes treatment, as products that will drive Merck sales going forward.
The company also hopes to recover some of the impending Zocor sales vacuum with the cholesterol drug Vytorin, which combines Zocor with Schering-Plough's (up $0.42 to $19.31, Research) Zetia. Launched in 2004, Vytorin sales totaled $2.4 billion in 2005 sales.
Barbara Ryan of Deutsche Bank North America said in a note that Merck's biggest challenge, the Vioxx liability, has already been baked into the stock price, which has been discounted for $30 billion worth of possible damages.
"We believe Merck has put in place an aggressive, but achievable strategic plan, and with a new management team that is motivated and determined to execute, with a new sense of urgency and accountability," wrote Ryan, who rates Merck a "buy" with a price target of $38.
David Moskowitz, analyst for Friedman, Billings, Ramsey, has projected the highest Vioxx damage estimate, at $50 billion.
--
To read about Big Pharma v. biotechs in year-to-date stock performance, click here.
The analysts interview for this story do not own Merck stock, but Deutsche Bank North America does seek business with them.
---------------------------------------------

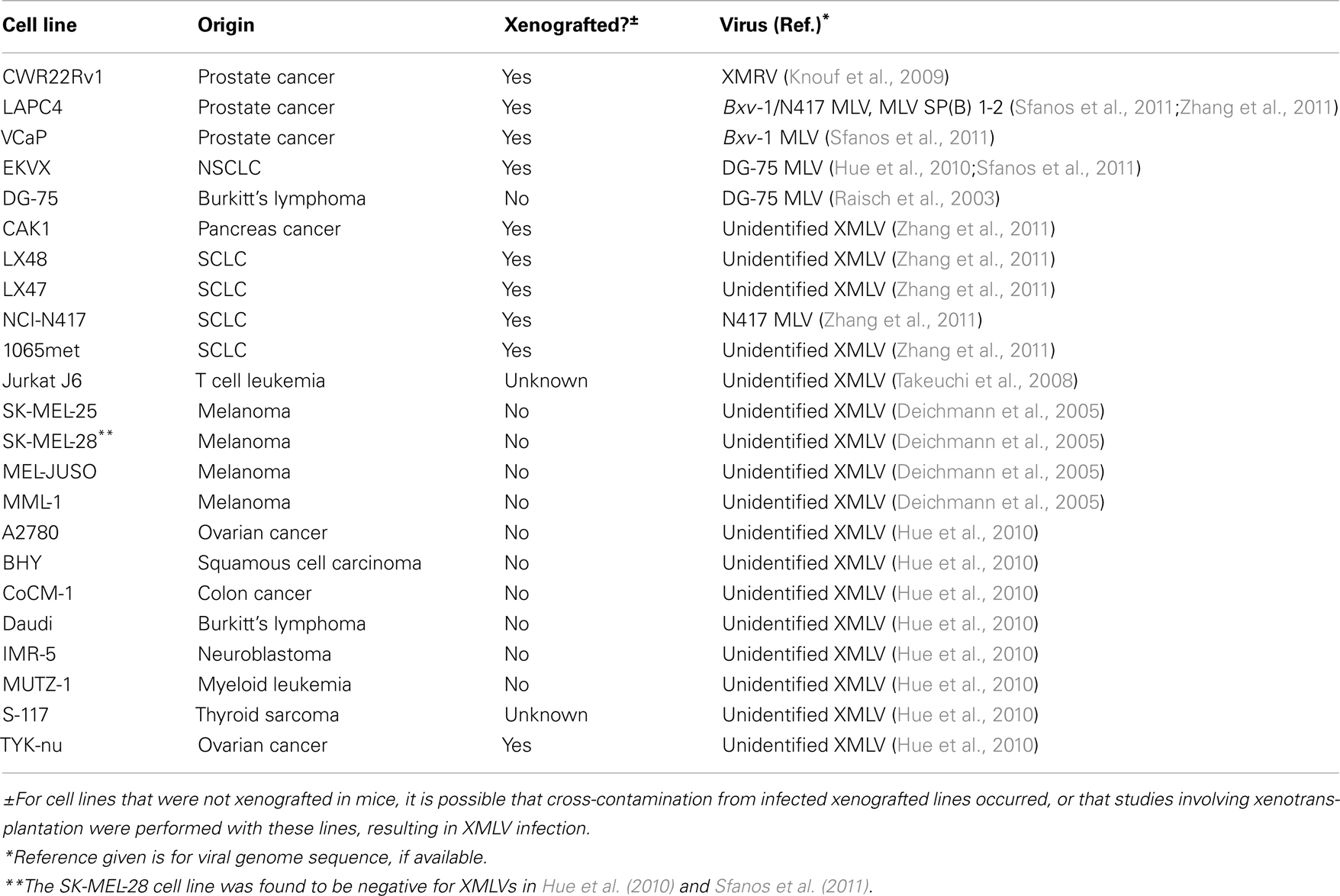{kind=link}
Robyn Erland copyright my wording - Here's and another posting I made on gardasil profits in 2016:
Robyn Erland
Mar 28, 2016 11:52 AM
who.int
Check this out. It's the WHO Global Vaccine Market information. And here are some of the highlights from it:
RAPID GROWTH and CHANGING STATUS
Tripled in value from USD 5 Billion in 2000 to almost USD 24 Billion in 2013
Global market projected to rise to USD 100 Billion by 2025
More than 120 new products in the development pipeline
Vaccines: becoming an engine for the pharmaceutical industry
hanging status of the vaccines within the pharmaceutical industry
New business model for vaccines is emerging?
Newer and more expensive vaccines are coming into the market faster than ever before
Vaccine development: increasing investment
2010 sales (US$)
Prevnar
-
13 (Pfizer) valent pnenumococcal
conjugate vaccine
$2.4 billion
Proquad (Merck/Sanofi-Aventis)
Measles - mumps -rubella and
varicella combination vaccine
(MMR - V)
$1.4 billion
Gardasil (Merck)
HPV
$1.35 billion
Prevnar (Pfizer)
valent pnenumococcal conjugate
vaccine
$1.2 billion
Fluzone (Sanofi Pasteur)
Influenza (seasonal and H1N1 strains)
$1.2 billion
Infanrix and Pediarix) (GSK)
Infanrix = DTaP
Pediarix = DTap - HepB - IPV
(combination DPT - based vaccines
with acellular pertussis)
$1.2 billion
You all really should take a look at these profits. And with zero liability for any harm done to anyone, it is a win win for the pharmaceutical manufacturers once the law was put in saying they could never be sued. Even for deaths they cause. It's also no wonder they have made even infants their newest clients. Zero liability with huge profit going into their fat pockets. And who pays the price for injuries or the diseases that come with their retrovirus lab recombinations that wound up in cell lines for decades? We do!!!
https://www.who.int/influenza_vaccines_plan/resources/session_10_kaddar.pdf?fbclid=IwAR0JzZWjw0ckcTf878KJ7n91mizsvL4iqvZKJyOzHwK-R9yisCpNBkfEt0I
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.